Egydio’s Technique: Know the Efficiency of Peyronie Disease Treatment
[EBOOK]
What is the Egydio's Technique?
In 1965, the American urologist, surgeon and professor, Dr. Reed Miller Nesbit, entered the history of medicine by introducing the only technique for correction of penile curvature known until then. Over the next few years, modifications appeared to treat a curved penis, such as Kelâmi-Nesbit1, Yachia2, Devine-Horton3, Sampaio, Gelbard4, Lue H5, among others, until, 55 years after the first successful method, came the principles Geometric procedures6,7,8, affectionately named by the national and international urological community as Egydio’s Technique6,7,8, or Egydio’s Geometric Incision6,7,8, or Egydio’s Technique6,7,8, or Egydio’s Geometric Procedure6,7,8, among other nomenclature variations.
She was described by Dr. Paulo Egydio, Brazilian physician PhD in Urology, in his doctoral thesis at the University of São Paulo (USP) in 2000 on the surgical treatment of Peyronie’s Disease.

This modification improved the methods already recognized and mentioned above and was incorporated into the correction statistics of diseases that cause deformities in the penis, such as Peyronie’s Disease and congenital curvature, which according to the Cleveland Clinic, affect between 6% and 10% of the population. male between 40 and 70 years old. Currently, it is present in the guidelines of the American Urological Association (AUA), European Association of Urology (USA) and Canadian Urological Association (CUA).
In this surgical strategy, geometric principles are used to correct the penile curvature and increase the short side. It defines the location and characteristics of the incisions in the tunica albuginea (tissue that covers the erection mechanism).
On an erect penis, if an imaginary straight line is drawn over it, it is possible to identify that the member begins to curve when it stops touching the straight line, and at how many different points this happens.
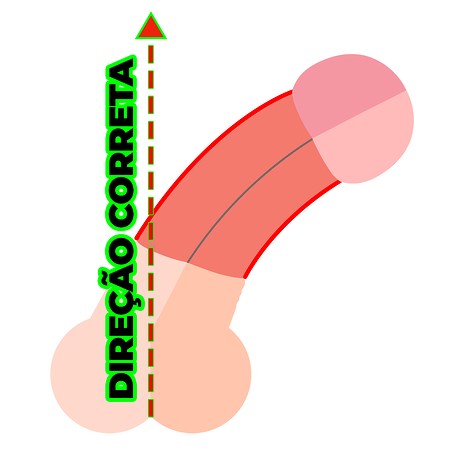
By adopting geometric principles, a surgeon is able to calculate the difference between the long side and the short side, and how much to lengthen the shortened side to make it the size of the longer one. After this calculation, it is possible to define the best strategy to be followed.
When performed according to geometric concepts, the accuracy for correcting diseases that cause penile deformities tends to be greater. According to the European Association of Urology (EAU – European Society of Urology), the technique helped to determine the exact point of incising, excising and grafting the penis.
These same principles can be applied to the so-called adjuvant maneuvers (reconstruction of the size and caliber of the penis at the time of penile prosthesis implantation). In this case, the multiple incisions aim to expand the tissues to the limits of the nerves, vessels and urethra, preparing the penis for receive an implant without the need to use grafts, if the defects (openings in the tunica albuginea) are smaller than 2 (two) centimeters.
This limit will only be known at the time of surgery, when the professional accesses the penile cylinder internally and checks the size of the nerves when compared to the size of the tunic . The recovery is done in such a way that this neurovascular bundle is still capable of being stretched to its maximum size, that is, it is limited by the anatomy of that patient.
Doubts? Send your question to Dr. Paulo and receive specific guidance about your condition, in a simple and discreet way.
Modified Egydio Technique
In medicine, over time, it is expected that the treatments available for the most diverse ailments evolve and change. With the Egydio Technique, it would not be different.
Surgeons, over time, used combined incisional maneuvers, guided by geometric principles, varying according to the specific characteristics of the deformities and fibrosis present in each particular patient, seeking better results.
In the more than 20 years of existence of this surgical strategy, which appears in the Guidelines (Guidelines) of the United States9, Europe10, and Canada11, as well as books used in the training of urologists in Brazil by the Brazilian Society of Urology (SBU), it has gone through modifications in its geometric principles,
in the applications and size of the incisions, which have been increasingly individualized and adapted to the case of the patient being operated on. In addition, due to the increasing precision of incisions, the method minimized the need to use grafts or artificial skin, which was the most traditional technique until then.
One of the recent contributions of Dr. Paulo Egydio was the chapter “A tunica expansion procedure (TEP): an innovative non-grafting proposal for penile enlargement (the Egydio TEP strategy)12”, present in the book “Peyronie’s Disease: Pathophysiology and Treatment”, awarded at the AUA-2019 American Congress of Urology, and which won the Chicago American Congress of Urology debate in 2019.
In it, the physician explains how the Tunica Expansion Procedure (Egydio TEP Strartegy) benefits from multiple, small incisions to promote tissue expansion and minimize the use of grafts. Thanks to this application of incisional maneuvers, there were improvements in the result and in the postoperative period when compared to other methods.
Doubts? Send your question to Dr. Paulo and receive specific guidance about your condition, in a simple and discreet way.
History of the Egydio Technique
The use of geometric principles to improve the precision and location of incisions during procedures already established for the surgical treatment of Peyronie’s Disease, associated or not with penile prosthesis implantation, is authored by Dr. Paulo Egydio,
specialist in urology and andrologist from the Faculty of Medicine of the University of São Paulo-USP. After graduation, the professional completed five years of medical residency at the Hospital das Clínicas of the University of São Paulo (USP), two years in general surgery and three years in urology, and completed specialization courses at the Mayo Clinic and at the Cleveland Clinic Foundation, in the U.S.
It was shortly after completing his residency at the Hospital das Clínicas, in 1996, that the doctor decided to dedicate himself to an area of concentration in penile surgery: solutions that could be given for the different types of fibrosis that give rise to Penile Disease. Peyronie.
The Doctor. Paulo then asked Professor Dr. Sami Arap, full professor and emeritus at the USP Faculty of Medicine, to create an outpatient clinic specialized in Peyronie studies at the Hospital das Clínicas of the USP Faculty of Medicine. Permission came in 1998 and, for eight and a half years, the professional worked as a volunteer at this outpatient clinic and became a specialist in the surgical treatment of Peyronie’s Disease.
The interest in this area of surgical concentration, combined with the experience in the outpatient clinic, gave rise to the doctoral thesis of Dr. Paulo Egydio, published in 2000. Entitled “Correction of penile deformity in Peyronie’s Disease with incomplete circumferential double Y6 incision”, the thesis is available on Research Gate, a social network focused on scientific publications.
What this thesis brought new to the surgical treatment of acquired penile curvature were the geometric principles. That’s how medicine evolves and that’s exactly what the Egydio Technique provided. The surgical procedure and the various types of incisions already existed, were consecrated and practiced by urologists before Dr. Paul Egydio. The surgeon applied for and obtained US and European patents on this method.
The introduction of geometric principles was due to the learning and experience that the author of the technique gathered throughout his undergraduate, residency and specialization years. Additionally, Dr. Paulo Egydio showed an interest in mathematics, in particular geometry, from childhood and, later on, was able to apply spatial, physical and biomechanical principles in medicine.
Prior to the description of the technique, traditional methods of treating Peyronie’s Disease did not precisely define the number, size, location and direction of the incisions needed to straighten the penis. With the application of geometric principles, the surgeon can calculate the best way and place to make the cuts in order to obtain better results in terms of rectification and/or size and/or caliber of the penis after the operation.
Recognition of the Egydio Technique
The contribution that geometric principles brought to penile curvature correction cases is proven worldwide.
The Regional Council of Medicine of São Paulo states that “the technique used by Dr. P.H.E. it is a modification of a surgical technique already established worldwide, and its contribution to its improvement is recognized and incorporated into the Peyronie correction statistics”. The full text is available in its Opinion nº 99.212/10.
The Brazilian Society of Urology (SBU), in the book UROLOGIA BRASIL, chapters 25 and 139, as well as the American Urological Association (AUA – American Society of Urology) and the European Association of Urology (EAU – European Society of Urology), widely recognize the Egydio Technique.
An example in this sense was the participation of Dr. Paulo Egydio in Survivor’s Debate,
promoted by the AUA in Chicago, United States, in 2019. In a hypothetical case of severe Peyronie’s Disease associated with Erectile Dysfunction, more than 70% of the 5 thousand urologists present in the audience agreed that surgical treatment adopting this surgical strategy was the best best option for the challenge presented.
The Egydio Technique is currently part of the guidelines that American9, European10 and Canadian11 societies use as a source of information, in order to standardize urologists’ conduct and decision-making for each type of penile deformity.
Consecration by the medical community
The medical community also recognizes the contributions of Dr. Paulo Egydio to medicine. In 2004, urologist Dr. Harris Nagler sent a letter to the urologist, and was the first to refer to the technique as Egydio’s Technique6.
In 2008 Mulhall J13. et al presented a study on incisions in the fibrosis plaque and named the surgical strategy from the geometric principles of Egydio’s Geometrical Incision 6. The study is published in the Journal of Urology of the American Urological Association.
In the Asian Journal of Andrology, Sansalone S. et al published in 2011 a multicentric European study14 with a series based on 157 patients who were operated using the geometric principles published by Dr. Paul Egydio. The technique used was also referred to as Egydio’s Technique.
In 2015, Konstantinidis K published a study15 in the Arab Journal of Urology with a sample of 330 patients surgically treated with the principles attributed to Dr. Paul Egydio. In this case, the method was referred to as Egydio’s Geometrical Procedure, (Egydio’s Geometrical Procedure).
Subsequently, other urologists around the world incorporated the technique into their activities and studies, referring to it as the Egydio’s Technique and variations – a way of supporting the doctor’s dedication and commitment in the treatment of diseases that develop fibrosis in the penis, such as Peyronie’s disease, post-radical prostatectomy penile retraction, diabetes retraction, and erectile dysfunction.
Doubts? Send your question to Dr. Paulo and receive specific guidance about your condition, in a simple and discreet way.
Nesbit X Egydio Technique
Nesbit technique, also called plication, consists of aligning the penis by making folds in the tunica albuginea, which reduce the long side of the penis.
This creates equality in size in relation to the short side, but at the same time causes the penis to decrease.

When Peyronie’s Disease causes the penis to thin, procedures performed with Nesbit will not solve the problem. A thinned penis has less penetrative resistance, creating a favorable environment for new fibroses to appear, causing new points of deformity, whether through thinning, curvatures or even reduction in the size of the penis.
With incisional maneuvers, guided by geometric principles, surgeons seek to recover the maximum size and caliber of the penis. The maximum size is limited by the nerves, vessels and urethra. This is possible thanks to the relaxation cuts made in the tunica albuginea, which geometrically cause longitudinal and/or transverse sliding.
When there is penile thinning, for greater expansion of the penile tissue, the incisions are made vertically in order to cause an expansion in the direction of the caliber (transverse sliding). In patients with size loss, horizontal incisions are applied to lengthen the penis to the limits of the nerves and urethra (longitudinal sliding).
In the Nesbit technique, for suturing the folds, a surgical thread that is non-absorbable by the body is used. If the wire comes loose, the curl returns. In addition, the wires can be felt through the patient’s skin and, in some cases, even hurt.
This inconvenience tends not to happen when the operation is performed with sutures that are absorbable through the skin. After healing, they are absorbed by the body and cease to exist.
Doubts? Send your question to Dr. Paulo and receive specific guidance about your condition, in a simple and discreet way.
Diseases treated by the Egydio Technique
The technique is widely used to surgically treat diseases that cause a reduction in size, tortuosity and/or thinning of the penis, with the possibility of recovering its size and caliber, in whole or in part.
Peyronie's disease
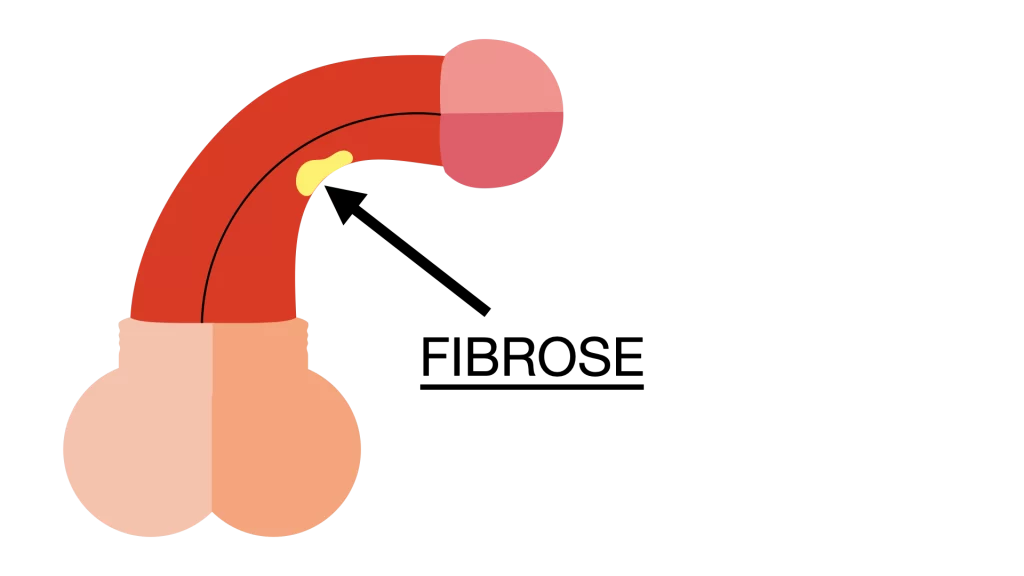
Peyronie’s disease, also called acquired curvature, it consists of a fibrotic process installed in penile tissues, which can generate tortuosity and/or thinning and/or reduction in penile size. Generally, these changes are noticed by the patient when the member is erect.
Peyronie is caused by the formation of one (or more) fibrosis plaque in the tunica albuginea. These fibroses can be consequences of traumas or microtraumas that happen throughout the man’s life, both during sexual activities and also in situations where the man forces the penis too much in erection. An example is the combination of an involuntary erection during sleep and a prone position or rolling the body on the mattress, forcing the erect penis to the point of causing microtrauma.
The origin of the fibroses that cause Peyronie’s Disease can be multifactorial and is still not exactly known.
The scarring of the fibroses causes the penile tissue to lose elasticity, which is why the deformity appears during an erection.
Curvature can evolve over time. In severe cases, the penis bends 90° or more. This anatomy makes it difficult or impossible to have a quality sex life, in addition to being able to cause pain during erection.
Risk factors
The disease tends to be seen more frequently in older men, as it is associated with erectile dysfunction, hormonal imbalance, blood flow conditions and some comorbidities. Although less frequent, they can occur in young patients as well.
Diabetes
blood glucose elevation– diabetes – also favors the onset of the disease, due to damage to the functioning of blood vessels and nerves. In this case, fibroses can form even if there is no trauma in the region. Furthermore, diabetes is one of the main causes of erectile dysfunction.
Symptoms
Most of the time, the patient himself notices that his penis is different. However, Peyronie’s Disease has a set of symptoms. It is the case of:
Tortuosity
The most noticeable symptom, tortuosity, depends on the location and scarring of the fibrosis in the tunica albuginea, in addition to the magnitude of the loss of tissue elasticity.
The penis can be bent sideways, upwards (towards the navel) or downwards. The most common among patients is the downward curvature. It is only noticed during erection.
Tuning
The patient may also notice, when the penis is erect, a thinning. This thinning can be hourglass-shaped (in a single place, circumferentially), indented (on one side only) or diffuse, with more than one point of thinning.
Penis with hourglass thinning
Penis with indentation thinning
Diffuse thinning penis
Difficulty in penetration
If penetration does not occur easily, it could be an alert for Peyronie’s Disease, especially when, even when adjusting the penis with the hand, the fit does not occur easily.
Penis bends or leaks
During intercourse, tortuosity can cause the penis to bend or slip out easily due to loss of vertical rigidity and decreased penis size. This can cause new traumas, which, in addition to discomfort, can aggravate Peyronie’s condition.
Pain or discomfort in the partner
If the tortuosity is more accentuated, even if the member is firm enough to maintain the erection, the partner may feel pain during penetration. This is because the sinuous anatomy is not favorable for the person who is penetrated.
Penis pain after intercourse
After completing the sexual act, even if the relationship has taken place without difficulties, the penis can be sore. This indicates that it is probably being improperly forced to conform to the curvature.
congenital curvature
Known as congenital curvature or curvature of the young man, this condition also causes penile tortuosity, noticed during erection. However, unlike Peyronie, which is acquired throughout life, the man is born with this discrepancy in elasticity between the sides of the penis when being pressurized into an erection.
Generally, the disease is identified during puberty, when penile development accelerates and erections happen more frequently.
This type of curvature is congenital in nature and occurs because one side of the penis has developed less than the other, that is, it is larger or more elastic compared to the opposite side, causing lateral tortuosity, upwards or downwards. , downwards being the most common.
Sometimes, the deformity does not prevent the patient from leading a satisfying sex life. If the man has sex with the penis well lubricated with specific products, avoids too sudden movements and carefully chooses the positions, he can live in harmony with the curvature.
However, the presence of any curvature makes the penis more susceptible to trauma during sexual intercourse, the main cause of Peyronie’s Disease, and congenital disease can evolve for a more serious picture.
Symptoms and early diagnosis
In addition to the apparent deformity of the penis, the curvature of the young man is accompanied by other symptoms that allow its identification.
Penetration in sexual intercourse can be a very difficult or even impossible experience. During the act, the penis is escaping, painful and can bend. The partner may also feel pain.
It is essential that the diagnosis be made by a urologist as soon as possible.
By moving ahead, it is possible to prepare the patient for corrective treatment in the future and instruct him to minimize the risks of worsening the disease and developing Peyronie.
Thus, compromising the young person’s sexual, psychological and social development can be avoided.
Despite this importance, the search for a professional often takes time to happen. Teenagers often feel a certain embarrassment when approaching the subject with their guardians, and end up postponing this conversation.
Doubts? Send your question to Dr. Paulo and receive specific guidance about your condition, in a simple and discreet way.
How is Peyronie's surgery done?
The surgical procedure for Peyronie’s Disease is the most appropriate option if clinical treatment is unsuccessful and the functional condition of the penis for penetrative sexual activity has been compromised by fibrosis or deformities.
Before being referred for surgery, the patient with Peyronie’s usually has already experienced one or more clinical treatmentss,
either with medication or with injections applied to the penis. These treatments aim to stabilize the disease so that it does not advance to a degree that hinders the penetrative capacity during the sexual act.
When the deformity continues to evolve or when it is already too advanced to be resolved with clinical treatment, the urologist will assess the indication for surgery. The indication may also come when the patient presents, in addition to tortuosity, thinning, erectile dysfunction and/or lack of penile firmness for the penetrative act.
Peyronie’s surgery aims to return to the penis its penetrative function, so that, at the right time, the man has enough rigidity to break the resistance and penetrate the partner. Its objective is not to increase the size of the member, although surgery with the Egydio Technique is capable of recovering penis measurements to some extent.
Incisional maneuvers or adjuvant maneuvers may be necessary to correct penile deformities, with the implantation of a prosthesis, in patients affected by Erectile Dysfunction and Peyronie’s Disease concomitantly, which may provide the size and caliber expansion and correction of deformities such as curvatures and thinning. What allows this resizing is the expansion of the tissues from relaxation cuts made based on the geometric principles described by the urologist Dr. Paul Egydio.
Before receiving the surgical indication, the patient who has some type of penile tortuosity must go through some stages – from the first appointment to, in fact, the procedure and recovery.
How is the query?
The first step towards the treatment of diseases like Peyronie’s, associated or not with erectile dysfunction, is to seek out a urologist, preferably one who has experience in this type of treatment, and make an appointment.
During the consultation, in general, the physician seeks to investigate the clinical history to understand the patient’s condition a little more. The information collected at this time may even be more relevant than the exams.
Some examples of the content of the conversation between doctor and patient are:
- How are your sexual relations with your partner?
- Has there been a change in the characteristics of the penis? (Size, thinning, curvature, etc.)
- Are you diabetic?
- Do you have cardiovascular disease?
- Do you continuously use any medication?
What exams can be ordered?
When the patient arrives at the office with complaints of penile tortuosity that has not been resolved with clinical treatments, the urologist will request additional tests.
They will help the physician to build an individualized surgical plan, aiming to obtain higher success rates and patient satisfaction after the procedure is completed.
The complementary exams and analyzes are the following:
drug-induced erection
With the help of medications, the doctor induces an erection to assess the erectile response of the penis and assess the degree of curvature in erection.
Vertical stiffness test
If an induced erection has been achieved, the vertical resistance of the limb is evaluated at this point. At this stage, it is possible to assess the ability to overcome the resistance that is imposed during penetration. If it is found that the penis bends easily, there are indications that vertical rigidity is compromised.
Penis inspection and palpation test
Depending on the case, the urologist can feel the fibrosis through palpation. The exam can also help identify which plaques compromise the rigidity of the penis.
penis ultrasound
O penis ultrasound it is one of the most important tests before surgery to correct Peyronie’s.
It better shows the situation inside the penis. Thus, it will be possible to discover the main characteristics of fibrosis, such as size, thickness and texture, for example.
Another valuable information that Doppler ultrasound provides is the analysis of blood flow in the arteries. In this way, the urologist determines whether there is arterial insufficiency or veno-occlusive dysfunction (the popular venous leak).
It is important to point out that this exam must be performed with the penis erect. This is the only way to assess the behavior of blood filling inside the penis.
How is the pre-op?
With the information collected in the clinical history, added to the results of complementary exams, once the patient has surgical indication, it is possible to start planning, discussed between doctor and patient.
At this stage, the surgeon presents the most appropriate surgical strategy for the patient’s deformity, in some cases, there is the possibility of having an Erectile Dysfunction associated with Peyronie’s Disease, and it is possible to associate the placement of a penile prosthesis implant, which will be done in the same surgical procedure – in this scenario, the conversation also includes discussions about the best type of prosthesis for the case in question.
Before surgery, the patient must undergo laboratory tests to prevent complications, especially if glucose levels are out of control, which increases the risk of infection and hinders healing.
The medical team will also provide guidance on cleaning the pubic area with an antibacterial soap, which needs to be properly performed before the surgery.
The patient will also need to fast for eight hours without ingesting solids or liquids.
How is the pre-op?
The procedure to treat Peyronie’s curvature usually lasts between 2 and 3 hours.
First, the pubic hair is shaved and then the patient receives sedation and local anesthesia.
Access way
The choice of access route is important to minimize the risk of infections.
In the case of surgery performed using the Egydio Technique as a strategy, the most indicated access route is the subcoronal, in which the skin of the penis is lowered, internal procedures are performed without touching the skin, minimizing the risk of infection. It’s the No-Touch technique.

Subcoronal incision “lowers” the skin
It is recommended that the physician use the No-Touch technique16, described by the American Dr. J. Francois Eid. With this, the graft (when indicated) and/or the implant will have very little contact with the patient’s skin, which contains bacteria, even after being washed and disinfected, especially in the scrotal region.
Incisões
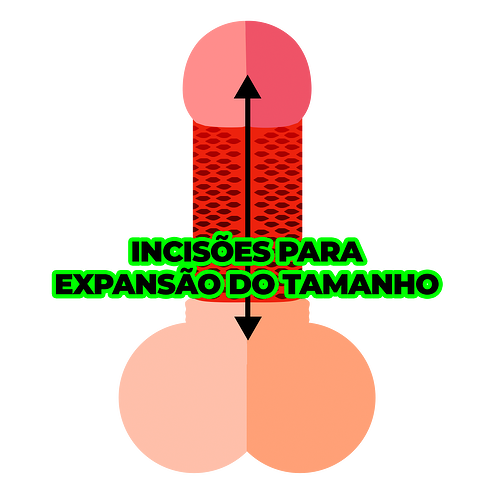
Após a dissecação dos nervos, múltiplas incisões de relaxamento são aplicadas para retificar o membro e aumentar o lado que diminuiu de tamanho, com base nos princípios geométricos. Isso permite reconstruir o pênis até o limite dos nervos e da uretra.
Quando o paciente tem indicação de implante de prótese peniana associado à correção da curvatura no pênis, pode ser necessário o uso das manobras adjuvantes para a expansão de tamanho, calibre e deformidades. As manobras são largamente aprovadas e usadas por especialistas, pela comunidade médica e pelas sociedades urológicas de todo o mundo.
As incisões são aplicadas no sentido perpendicular à direção da expansão. Ou seja, se queremos que o pênis recupere tamanho, os cortes são feitos na horizontal; para recuperar calibre, os cortes são verticais. Geralmente quanto maior o número de cortes, mais o tecido se expande. O objetivo é produzir a expansão necessária criando defeitos pequenos.
Graft
The use of geometric principles improved precision and the most favorable place to apply it, resulting in smaller “defects” (openings) in the tunica albuginea. When they are smaller than 2 (two) centimeters, the literature indicates that the use of grafts can be dispensed with, depending on the decision of each surgeon.
In addition to bringing a greater risk of infection, the use of grafts limits the recovery of size and caliber, can create an aesthetic defect (“patchwork” effect) and requires long suture lines, which are not absorbed by the body and can be perceived throughout life.
Como é o pós-cirúrgico?
No post-surgery of Peyronie’s surgery the patient returns to the doctor for evaluation and receives guidance, such as the use of a bandage in the first five days, and later changing it daily.
Depending on the work activity and the evolution of each patient after surgery, on average, the recovery phases are:
- Between five and seven days it is already possible to return to work.
- 30 days after surgery, the patient returns to physical exercises.
- Between 45 and 60 days, after a new medical evaluation, he is discharged to resume his sexual life.
- Surgical stitches are absorbed in up to two months.
*Dates may vary according to the recovery process of each patient, upon medical evaluation.
congenital curvature
Known as congenital curvature or curvature of the young man, this condition also causes penile tortuosity, noticed during erection. However, unlike Peyronie, which is acquired throughout life, the man is born with this discrepancy in elasticity between the sides of the penis when being pressurized into an erection.
Generally, the disease is identified during puberty, when penile development accelerates and erections happen more frequently.
This type of curvature is congenital in nature and occurs because one side of the penis has developed less than the other, that is, it is larger or more elastic compared to the opposite side, causing lateral tortuosity, upwards or downwards. , downwards being the most common.
Sometimes, the deformity does not prevent the patient from leading a satisfying sex life. If the man has sex with the penis well lubricated with specific products, avoids too sudden movements and carefully chooses the positions, he can live in harmony with the curvature.
However, the presence of any curvature makes the penis more susceptible to trauma during sexual intercourse, the main cause of Peyronie’s Disease, and the congenital disease can evolve into a more serious condition.
Symptoms and early diagnosis
In addition to the apparent deformity of the penis, the young man’s curvature is accompanied by other symptoms
that allow your identification.
Penetration in sexual intercourse can be a very difficult or even impossible experience. During the act, the penis is escaping, painful and can bend. The partner may also feel pain.
It is essential that the diagnosis is performed by a urologist as soon as possible.
By moving ahead, it is possible to prepare the patient for corrective treatment in the future and instruct him to minimize the risks of worsening the disease and developing Peyronie.
Thus, compromising the young person’s sexual, psychological and social development can be avoided.
Despite this importance, the search for a professional often takes time to happen. Teenagers often feel a certain embarrassment when approaching the subject with their guardians, and end up postponing this conversation.
Doubts? Send your question to Dr. Paulo and receive specific guidance about your condition, in a simple and discreet way.
When is the penile prosthesis implant indicated?
It is usually indicated for situations in which the patient arrives at the doctor’s office with Peyronie’s Disease and also presents erectile dysfunction and/or lack of rigidity for penetrative sexual activity. The diagnosis takes into account the symptoms of the disease and that can be proven with the clinical history, erection induction, the vertical rigidity test and the Doppler ultrasound.
What happens is that poor quality erections and/or small penile traumas, throughout life, can cause fibrosis in one point or several points of the limb, and are responsible for tortuosity and/or thinning and/or size reduction. These complications and deformities cause the limb to lose resistance to penetrative sexual activity. As a result, during penetration, the penis can easily bend or escape, which generates new trauma and new fibrosis. This condition can drastically impact the quality of male sexual life, both for physical reasons, which hinder or prevent penetration, and for generating psychological problems resulting from Peyronie’s disease itself and deterioration of mental health.
With the objective of giving the man the vertical support that the penis needs for the sexual act, the medical recommendation can be a penile prosthesis implant,
which can be performed in the same surgery that treats the fibrosis and reconstructs the limb.
In addition to treating the vertical rigidity deficit, the penile implant aims to prevent new fibrosis. With better rigidity, the penis is less subject to trauma or micro trauma, which sometimes happen during sexual intercourse.
When the prosthesis is not placed, there are chances that the fibrosis will reappear and a penile prosthesis implant is not intended to enlarge the penis.
By using geometric concepts, the surgeon’s main objective is to place a larger and thicker prosthesis. This strategy aims to result in a penis with greater vertical rigidity, size and caliber, that is, what increases the penis is the method chosen, and not the penile prosthesis, regardless of the model, malleable or inflatable.
By maximally expanding the tissues with adjuvant maneuvers, the penis will be able to receive a prosthesis of greater length and greater caliber, compatible with the patient’s new anatomy, since the relationship between length and caliber is essential for adequate penetrative function and better biomechanical relationship.
This is why even the introduction of the prosthesis, without reconstruction of size and caliber, may not meet expectations in terms of size, caliber and rigidity. A very long penis that has become thinner due to Peyronie’s Disease, for example, needs a larger caliber implant after its size has recovered, with improved axial resistance for penetration.
The internal structures of the penis, on the other hand, must be preserved as much as possible, aiming at greater blood flow. This allows – in addition to the penile prosthesis – a greater residual filling.
It is also necessary to be careful with the positioning of the implant: if poorly placed and/or sized, the cylinders can put pressure on the urethra causing pain, destroy the sponge of the cavernous bodies too much, not provide stability to the glans and not generate the necessary firmness (because it is too fine) for the penetrative sexual act.
Type of penile prosthesis
Currently, medicine has a highly developed technology with regard to penile prostheses. The predominant models are malleable (semi-rigid) and hydraulic (or inflatable).
The decision for the best type of prosthesis depends on a pre-evaluation at the time of the appointment. To do this, the surgeon takes into account factors such as the patient’s preference, anatomy, lifestyle and budget.
Malleable or semi-rigid prosthesis
Made of malleable silicone, which covers two metal rods, this prosthesis model offers good rigidity and malleability for the penis. It can be accommodated down, to the side, towards the groin, in an upright position (for the sexual act), just handling it with the hands. However, she does not allow penile flaccidity.
An advantage of malleable prosthesis is that it is covered by most health plans. It is also more affordable if the patient needs to make the purchase on their own.
Compared to the inflatable implant model, the malleable version has a lower failure rate. Thus, there are no risks of leaks, and the best thing is that it doesn’t stop working suddenly. When compared with the inflatable, the incidence of exchange is also lower.
There are several calibers of malleable prostheses. They must be chosen after penile reconstruction, according to the compatibility of cavernous bodies, so that the largest caliber is selected for each penile anatomy and adjusting the size in order to provide malleability and rigidity for penetration.
Hydraulic or inflatable prosthesis
hydraulic prosthesis it can have two or three volumes, depending on the model chosen, which are pressurized by activating a saline pump housed in the scrotum. When activated, the liquid goes to the cylinders, the prosthesis inflates and the patient gets an erection.
The great advantage is that, after the sexual act, it is possible to resume penile flaccidity by deflating the pump, leaving the member more discreet under the clothes than a penis that has a malleable prosthesis.
However, according to a study conducted by specialists from the University of Ankara in 2007 17, the hydraulic prosthesis has a higher failure rate than the malleable one. Its sophisticated system is more subject to mechanical failures caused by leakage of liquid from the reservoir, blockage of the pump and loss of resistance of the cylinder walls. If one of these situations occurs, it is necessary to undergo a new surgery for the replacement.
In addition to mechanical failure, the hydraulic prosthesis has a high cost and is not offered by most health plans. It is also worth remembering that patients who do not have manual dexterity will have difficulty handling the prosthesis, which is why it is not recommended for everyone.
What is it like to live with a penile prosthesis?
After leaving the hospital, the patient will go through a period of adaptation to his new prosthesis, after receiving the necessary instructions from the doctor.
About a month and a half or 60 days after surgery, the man is usually discharged to have sex again. He will notice a positive change in his penetrative rigidity, which tends to be adequate to overcome the resistance imposed by his partner at the time of penetration.
The prosthesis does not tend to impact the natural functions and sensations of the member, such as pleasure, orgasm and ejaculation. On the contrary: the implant aims to provide a satisfactory and healthy sexual routine.
Many men are concerned about the temperature and sensitivity of the penis after the operation. If the internal structures are properly preserved and the cylinder(s) of the implant is(are) well positioned, there is a greater possibility of having a residual erection during erotization.
Doubts? Send your question to Dr. Paulo and receive specific guidance about your condition, in a simple and discreet way.
Egydio Technique Before and After
The use of geometric principles to determine the best place to perform the incisional maneuvers, present in the concepts of the surgical strategy “dubbed” the Egydio Technique, tends to improve the results of correction of penile deformities and allows the implantation of cylinders with better positioning below the glans and cylinders of greater size and caliber, providing better functional and aesthetic results.
In general, surgeons, when applying all their knowledge, expertise and using geometric principles, aim to achieve
Alignment
The Peyronie and curvature of the young man causes the tortuosity of the penis. When corrected with the Egydio Technique, thanks to the treatment of the short side, using geometric principles, the doctor manages to lengthen this side, making it the size of the long side, as close as possible to the penis, minimizing the loss of size.
The physician’s experience in the pre, intra and postoperative period is crucial for a treatment approach that is more in line with the expectations of each patient. In some cases, the long side may also be affected, but to a lesser extent, therefore, there may be a need for tissue expansion not only on the short side, but also on the long side, which provides a better functional and aesthetic result.
Size
Surgical treatment consists of relaxation incisions that allow tissue expansion, recovering the size of the penis up to the limits of the nerves and urethra.
When indicated, it is possible to place a penile prosthesis of a larger size and greater caliber for the penis with dimensions recovered to the limit of what is possible.
Therefore, the member may be larger in size compared to the penis when affected by the curvature.
Thickness
If the surgery is performed with penile reconstruction associated with the implantation of the prosthesis, there are conditions for the surgeon to insert an implant of a larger size and caliber in the penis. This means that the specialist will expand the refined points to allow the entry of a thicker prosthesis.
In this way, the penile thinning is corrected, and the member will be more homogeneous compared to the penis affected by fibrosis and thinned.
The caliber of the prosthesis aims to give greater penetrative rigidity to the man. If the reconstruction is not done, the surgeon will probably be able to place a thinner prosthesis on this penis that is already thinned, and, in many cases, it will not be enough to give rigidity to the member during penetration.
Sensitivity
With the preservation of the bundle of nerves at the time of surgery, the sensitivity of the glans tends not to change.
Remembering that in a normal penis or with penile prosthesis implant, sensitivity should not be evaluated by simply touching the penis, such as, for example, in case of hygiene. The best way to assess penile sensitivity, especially of the glans, the most sensitive area of the penis, is under full erotization, which depends on brain activity for sex.
Orgasm
The objective of the surgery is to restore penile functionality, correcting deformities and/or providing penetrative capacity and rigidity for sexual activity, preserving as much as possible the nerves responsible for sensitivity. Under eroticization, the tendency is that there is no interference in orgasm and pleasure. In addition, in the case of penile prosthesis implantation, as it confers penetrative rigidity, it is possible to continue the sexual act for a longer time, even after the man has had an orgasm.
The volume and quality of the ejaculate also tend to be maintained, as the treatment does not change the structure that transports the semen.
With a penis that is more rigid and suitable for penetration, the patient tends to be more confident during intercourse, and this naturally reflects on the quality of his sex life and mental health.
In order to guarantee ethical conduct in the practice of medicine, the Federal Council of Medicine (CFM) prohibits the dissemination of “before and after” images on the Internet. Therefore, it is not allowed and it is considered an ethical infraction to disclose images on the Internet and/or on social networks. Patients should be wary of urologists who propagate this type of image.
Doubts? Send your question to Dr. Paulo and receive specific guidance about your condition, in a simple and discreet way.
References
1 – Kelâmi A. Congenital penile deviation and its treatment with the Nesbit-Kelâmi technique. Br J Urol. 1987;60(3):261-263. doi:10.1111/j.1464-410x.1987.tb05496.x
2 – Yachia D. Modified corporoplasty for the treatment of penile curvature. J Urol. 1990 Jan;143(1):80-2. doi: 10.1016/s0022-5347(17)39871-3. PMID: 2294269.
3 – Gelbard MK. Relaxing incisions in the correction of penile deformity due to Peyronie’s disease. J Urol. 1995 Oct;154(4):1457-60. PMID: 7658558.
4 – Gelbard MK. Relaxing incisions in the correction of penile deformity due to Peyronie’s disease. J Urol. 1995 Oct;154(4):1457-60. PMID: 7658558.
5 – Lue TF, El-Sakka AI. Venous patch graft for Peyronie’s disease. Part I: technique. J Urol. 1998 Dec;160(6 Pt 1):2047-9. doi: 10.1097/00005392-199812010-00029. PMID: 9817320.
6 – Egydio PH, Lucon AM, Arap S. Treatment of Peyronie’s disease by incomplete circumferential incision of the tunica albuginea and plaque with bovine pericardium graft. Urology. 2002 Apr;59(4):570-4. doi: 10.1016/s0090-4295(01)01651-x. PMID: 11927316.
7 – Egydio PH, Lucon AM, Arap S. A single relaxing incision to correct different types of penile curvature: surgical technique based on geometrical principles. BJU Int. 2004 Nov;94(7):1147-57. doi: 10.1111/j.1464-410X.2004.05220.x. PMID: 15541152.
8 – Egydio PH. Correção da deformidade peniana na Doença de Peyronie com incisão circunferencaial incompleta em duplo Y na placa e enxerto de pericárdio bovino. 2000. Tese (Doutorado)- Faculdade de Medicina, Universidade de São Paulo – Departamento de Cirurgia, São Paulo, 2001. USP/FM/SBD=257/00
9 – Nehra A, Alterowitz R, Culkin DJ, Faraday MM, Hakim LS, Heidelbaugh JJ, Khera M, Kirkby E, McVary KT, Miner MM, Nelson CJ, Sadeghi-Nejad H, Seftel AD, Shindel AW, Burnett AL; American Urological Association Education and Research, Inc.,. Peyronie’s Disease: AUA Guideline. J Urol. 2015 Sep;194(3):745-53. doi: 10.1016/j.juro.2015.05.098. Epub 2015 Jun 9. PMID: 26066402; PMCID: PMC5027990.
10 – Salonia A, Bettocchi C, Boeri L, et al. European Association of Urology Guidelines on Sexual and Reproductive Health-2021 Update: Male Sexual Dysfunction. Eur Urol. 2021;80(3):333-357. doi:10.1016/j.eururo.2021.06.007.
11 – Bella AJ, Lee JC, Grober ED, Carrier S, Benard F, Brock GB. 2018 Canadian Urological Association guideline for Peyronie’s disease and congenital penile curvature. Can Urol Assoc J. 2018 May;12(5):E197-E209. doi: 10.5489/cuaj.5255. Epub 2018 Feb 22. PMID: 29792593; PMCID: PMC5966931.
12 – Egydio PH. A tunica expansion procedure (TEP): an innovative non-grafting proposal for penile enlargement (the Egydio TEP strategy). In: Russo G, Cocci A (eds). Peyronie’s disease: pathophysiology and treatment. Academic Press: Elsevier Inc.; 2020. pp. 199–218.
13 – Flores S, Choi J, Alex B, Mulhall JP. Erectile dysfunction after plaque incision and grafting: short-term assessment of incidence and predictors. J Sex Med. 2011;8(7):2031-2037. doi:10.1111/j.1743-6109.2011.02299.x
14 – Sansalone S, Garaffa G, Djinovic R, et al. Long-term results of the surgical treatment of Peyronie’s disease with Egydio’s technique: a European multicentre study. Asian J Androl. 2011;13(6):842-845. doi:10.1038/aja.2011.42
15 – Konstantinidis K, Kuehhas F, Papatsoris A. The Egydio geometrical procedure for managing penile curvature using a single relaxing incision: A single-centre experience with 330 patients. Arab J Urol. 2015;13(4):287-290. doi:10.1016/j.aju.2015.08.001
16 – Eid JF. Penile Implant: Review of a “No-Touch” Technique. Sex Med Rev. 2016;4(3):294-300. doi:10.1016/j.sxmr.2016.01.002
17 – Akand M, Ozayar A, Yaman O, Demirel C. Mechanical failure with malleable penile prosthesis. Urology. 2007;70(5):. doi:10.1016/j.urology.2007.08.005
PEYRONIE'S EBOOK
Knowledge is the first step in carrying out a treatment, and there is nothing better than learning from an expert on the subject: Dr. Paul Egydio. The Peyronie’s Disease Guide is available for download and can also be consulted topic by topic below.
